Navigating Picky Eating in Kids with Food Allergies: The Ultimate Parent’s Guide
This post was initially published on May 27, 2026. You can also request a PDF copy of this Ultimate Guide.
Is your child a picky eater?
Have you been told that they’ll just eat when they’re hungry? Or that picky eating is a behavioral issue or phase they will outgrow?
I get it! There is so much well-intended yet misleading advice when it comes to picky eating.
For many kids – especially those with multiple food allergies – picky eating can actually be the first sign of a feeding problem.
This comprehensive article will explain what picky eating is, when to be concerned, how to navigate selective eating, and tips for feeding picky eaters.
Table of Contents
What is picky eating?
Surprisingly, picky eating is not easy to define.
There is no universal definition within the field of pediatric feeding therapy. Picky eating is not an ICD-10 medical diagnosis.
Instead, picky eating is a term generally used to describe those that:
eat a limited variety of foods,
are reluctant to try new foods, or
have strong preferences for taste, texture, and/or food preparation.
Picky eating is also known as selective eating or fussy eating. Other terms like finicky or particular are options with less stigma attached to them.
How common is it?
In the United States, caregivers report 19% of four-month-olds and up to 50% of two-year-olds are picky eaters. (1)
Another study suggests that 20% of children between two and six years old have moderate or severe selective eating. (2)
Remember, there is no standard definition for picky eating. This makes it more difficult to determine its exact prevalence.
For example, if a study uses a more general description of picky eating, the data could imply it is more prevalent. On the other hand, it would appear less common if more stringent criteria are used to define picky eating.
Regardless, we know that many kids (especially toddlers) are picky eaters. The next question is, why?
What causes picky eating?
In my clinical experience, picky eating is usually not caused by the parents.
There is research that supports this. A 2008 study found that feeding problems were not associated with parenting practices or poor feeding techniques. Instead, picky eating is caused by a combination of:
biological factors
sensory processing and texture aversions
psychological factors, and
medical conditions. (3)
For some kids, picky eating is just a phase. About one third of children who are picky at either 18 months or three years will outgrow it by age six. (4)
But only 8% of picky eaters will outgrow it by their sixth birthday if they are reported picky at both 18 months and three years. (4) And some of the pickiest kids will get even more selective over time. (5)
So if you are a parent of a picky eater, should you be concerned? How do you know if your child will outgrow it, remain picky, or become more selective?
What is the difference between picky eating and Pediatric Feeding Disorder?
Sometimes what appears to be picky eating is actually the tip of the iceberg for underlying feeding problems or developmental concerns.
In 2021, Pediatric Feeding Disorder (PFD) became a medical diagnosis with its own ICD-10 code, in large part due to the advocacy work of a group called Feeding Matters.
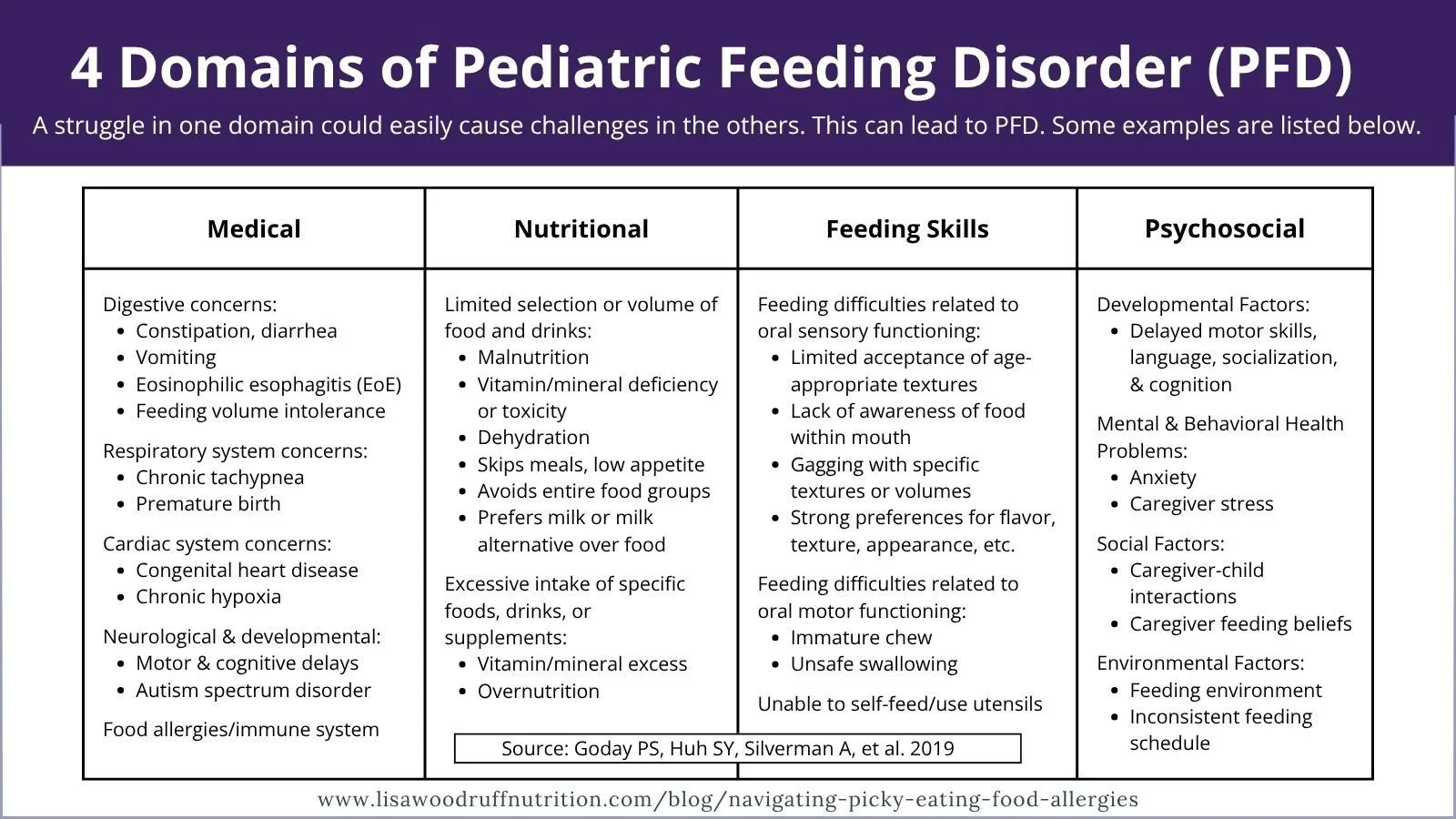
PFD is defined as an “impaired oral intake that is not age-appropriate, and is associated with medical, nutritional, feeding skill, and/or psychosocial dysfunction. (6)
Feeding is a complex process that involves interactions between an individual’s organ systems, sensory processing, development, environment, learning capacity, and nutritional status. Because these factors are interconnected, a struggle in any one area can easily cause challenges in the others.
Some examples of possible feeding challenges that could occur in the four domains are listed in the box below. Medical conditions most likely to impact feeding in children under five years include respiratory, gastrointestinal, prematurity, congenital, neurological, and cardiac disorders. (7)
Compared to picky eating, PFD is usually more complex. Children with PFD have a smaller amount of food preferences and may avoid entire food groups or categories of food. They are also more likely to have a meltdown when new foods are introduced and take longer to eat new foods.
Additionally, PFD often requires a multidisciplinary treatment team. This could include a registered dietitian for nutrition and occupational or speech language pathologist that specialize in feeding therapy.
Why is picky eating a concern in kids with food allergies?
Kids with food allergies are more likely to have feeding concerns than those without allergies. (8) And as the number of food allergies increases, the chance of also having a feeding difficulty also increases. (9)
Picking eating after 14 months of age is associated with:
having a lower enjoyment of food
being less likely to eat when upset at meals or snacks
having a higher desire to drink milk than eat table food. (10)
The addition of food allergies can place selective eaters at a higher risk for nutrition concerns and growth faltering.

Fear of trying new foods
When a family is learning how to manage a new food allergy, introducing new foods can be scary and overwhelming.
A parent’s anxiety during meals is directly correlated to how confident they are in managing their child’s food allergy. Concerns can quickly snowball over constant risk of allergen exposure and the impact on their child’s quality of life.(11)
The unfortunate result is that parents can unintentionally condition a fear response that any unfamiliar food is unsafe.
Kids that are afraid to try new foods tend to eat fewer foods. (12) And when kids have a smaller food range, it becomes even more difficult to expose them to a wide variety of foods, textures, and flavors.
Texture and sensory limitations
Trying new foods is an important step for young children to learn how to eat a wide variety of foods. There is a developmental window during which infants and young toddlers are most willing to try new textures.
Those who have learned to associate discomfort or pain with eating (like during a food allergy reaction) may come to prefer highly predictable, safe textures. As a result, they may start to reject anything unfamiliar or complex.
Safe alternatives to foods that contain allergens may have slightly different tastes or consistencies. And some foods, like peanut butter, have a very distinct taste and texture that is difficult to replicate outside of other nut butters.
When texture and sensory limitations further decrease food selection, the risk for nutrition concerns increases.
Nutrient insufficiency
Kids with multiple food allergies have a higher risk for micronutrient deficiencies.
Children that eat a larger variety of foods are more likely to meet their vitamin and mineral needs than those with a limited diet. (13) The cornerstone of food allergy management is allergen avoidance. But when entire food groups or types of food are eliminated, there is an increased risk for nutrient insufficiency.
Many of the Top 9 Food Allergens are found in core food groups. Avoiding common allergens like milk, egg, wheat, and soy can impact intake of nutrients like energy, protein, calcium, iron, and more.
Growth concerns
For many young kids, the onset of food allergy occurs at the same time as rapid growth.
An international study of children with food allergies found:
9% had stunted height
6% were underweight
5% were malnourished.
Additionally, those with EoE or FPIES were more likely to have lower height on growth charts. (14)
Adolescence is another stage of life when nutrition is crucial to optimize growth. There is an increased need for nutrients like calcium, magnesium, protein, and energy, as well as iron for girls. The combination of multiple food allergies and selective eating can make getting adequate nutrition even more difficult during this time.
It is important to note that kids with food allergies are at increased risk for poor growth, but not all kids with food allergies will have poor growth.
Pressure to eat
The more that parents pressure a child to eat, the more likely a child will refuse to try new foods. This becomes a vicious cycle, because parents are more likely to pressure a child to eat if they are a picky eater. (15)
Parents are also more likely to pressure their child to eat if they have concerns about weight gain. (16)
The combination of dietary elimination, feeding difficulties, inadequate nutrition, and growth concerns can unintentionally lead parents to pressure their child to eat. This is concerning because it can lead to mental health implications.
What is the difference between picky eating and ARFID?
Avoidant/Restrictive Food Intake Disorder (ARFID) is a broad term that describes several eating or feeding-related problems.
Unlike picky eating, ARFID is a clinically diagnosed eating disorder. It was included in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) in 2013. Those with ARFID often have severely restricted food intake due to:
Low appetite, lack of interest in food, or difficulty with the act of eating
Sensory problems or food aversions
A deep fear of aversive consequences of eating, such as choking, pain, or nausea. (17)
ARFID is a chronic condition that interferes with daily functioning and quality of life. This could look like avoiding social situations due to paralyzing anxiety and fear of new foods.
Children with ARFID have an increased risk for:
nutrition deficiencies
growth concerns
dependence on tube feeding or nutrition supplement drinks
the need for hospitalization related to malnutrition. (17)
Additionally, ARFID can negatively impact social and emotional development. As with other eating disorders, treatment requires a multidisciplinary team including primary care providers, psychiatrists, psychologists, nurses, dietitians, and occupational therapists.
What to do if you have concerns about your child’s eating
Here are some steps to help you take action if you have concerns about picky eating in your child with food allergies:
Step 1: Take the six-question screener (or the full questionnaire) available on the Feeding Matters website. If two or more answers are flagged, then please discuss your results with your child’s pediatrician or primary care provider. More information and resources are available from Feeding Matters.

Step 2: Make a list of all the different foods that your child is currently eating in each food category: protein, starchy foods, and fruit/vegetables.
These should be foods that your child eats most of the time; do not include foods they sometimes eat or are no longer eating.
Be specific! Instead of chicken, write down all forms of chicken that your child eats (chicken nuggets, shredded chicken, deli chicken, etc.).
Step 3: Count the total number of foods that your child is currently eating. Is the number less than 30? Or are there any categories with only a few foods? Or no foods at all? If so, your child might benefit from further evaluation by a pediatric dietitian or feeding specialist.
Step 4: Think about what happens when your child is offered a new food. Can they tolerate it on their plate or close by on the table? Or do they regularly melt down when something new is presented? If so, your child might benefit from further evaluation by a feeding specialist or pediatric dietitian.
Step 5: Now consider your child’s food allergies. Do they have a milk allergy or multiple food allergies? Are you struggling to find a variety of safe and appropriate substitutions? Or have you gotten behind in introducing new foods? All of these situations would suggest your child might benefit from further evaluation by a pediatric food allergy dietitian.
How to find a food allergy dietitian near you

A pediatric dietitian understands the developmental milestones involved with growing and learning how to eat. Dietitians with additional training in feeding therapy will focus on the how and why of eating; not just what to eat.
Furthermore, a pediatric food allergy dietitian can help:
Identify safe alternatives
Recognize possible nutrient deficiencies
Create a patient-centered plan to introduce new foods.
Working with a food allergy dietitian can improve both growth parameters and nutrition status. (18)
Food Allergy Research & Education (FARE) allows you to search for a FARE Trained Registered Dietitian in your state.
Are you in the state of Iowa? If so, I can help! I am a FARE Trained Registered Dietitian with experience in helping children with feeding concerns.
Click here to schedule an appointment.
As part of the initial assessment, I complete a thorough review of:
nutrition-related medical history
feeding history
developmental eating skills
mealtime structure
current food preferences, and
growth assessment.
After the visit, parents receive a report that includes any information on vitamins or minerals of concerns, appropriate substitutions for allergens, and additional resources for meal planning and food allergy management.
Tips for feeding picky eaters
There are many different philosophies when it comes to working with picky eaters. I tend to favor the approaches that value autonomy and help nourish a healthy relationship with food and eating.
For example, the Division of Responsibility in Feeding is an approach that defines specific roles for both parents and children. It honors a child’s natural ability to eat as much as they need, in order to grow in the way that is right for them.
Parents are responsible for what foods will be served, when meals are offered, and where the food is provided.
Children are responsible for how much to eat and whether or not to eat each food that is offered.
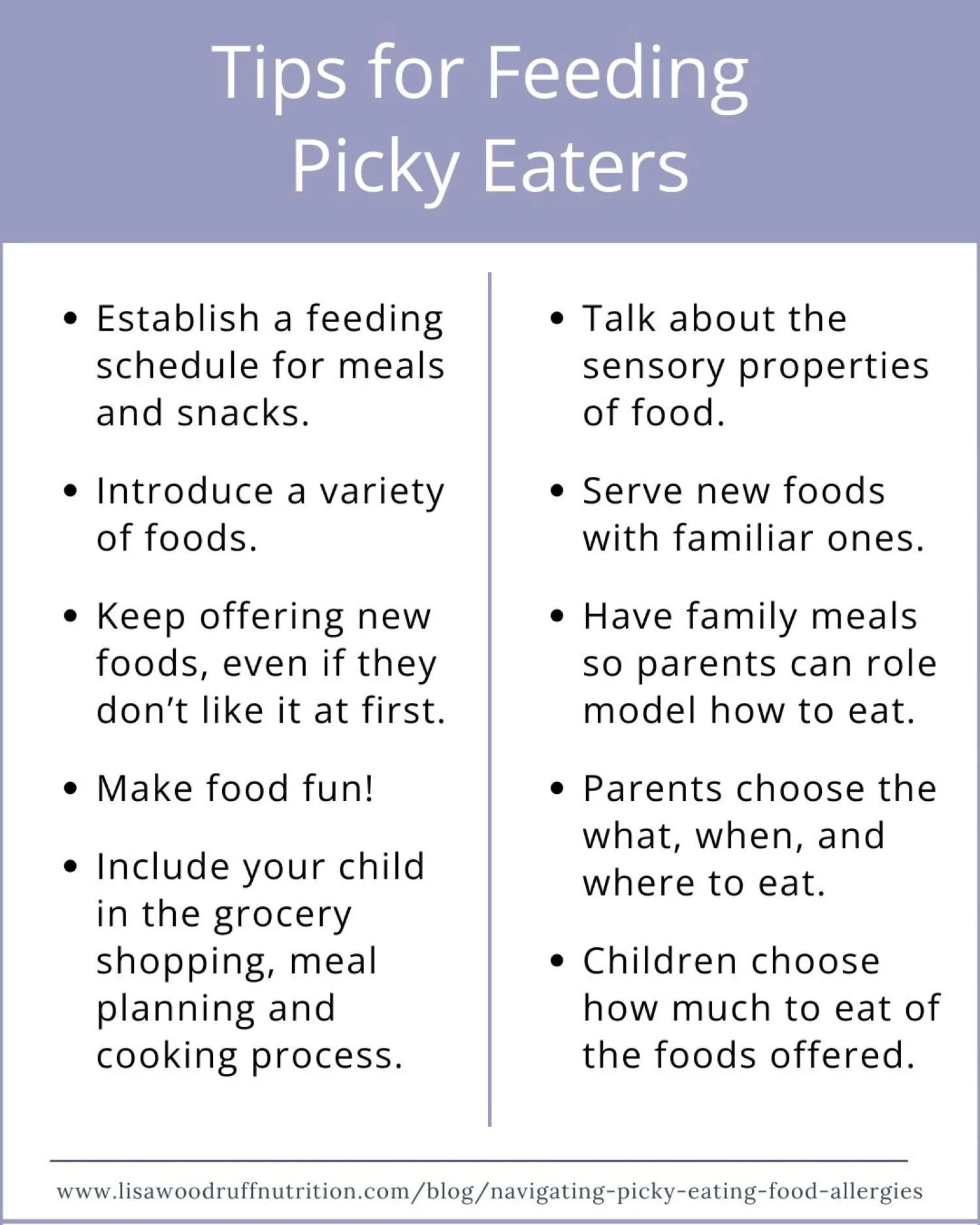
Here are some additional tips to help you feed your picky eater:
Establish a feeding schedule with designated meal and snack times.
Introduce a variety of food from all the food groups.
Keep offering new foods - sometimes it can take up to 10-20 exposures (or more) before a child feels comfortable trying something new.
Make food fun by including your child in the meal planning and food preparation.
Talk about the sensory properties of food during the meal instead of focusing on what your child is (or isn’t) eating.
Serve new foods with familiar ones (try a deconstructed meal).
Offer regular family meals so adults can role model desired eating habits.
When introducing new foods, remember to check every label, every time as products can (and do) change:
Read ingredient lists for allergens or check for a Contains statement.
May contain statements and other Precautionary Allergen Labels are voluntary and unregulated.
Certified allergy-free products and Nut-free facility labels are helpful, but always double check the ingredient list!
Final thoughts
Picky eating is a general term used to describe children that are selective with their food choices, reluctant to try new foods, and have strong taste or texture preferences.
It is different from Pediatric Feeding Disorder and ARFID, which are both medical conditions that require diagnosis by a doctor.
While some kids will outgrow their picky eating, others will become even more selective. If you have concerns about your child’s eating, a pediatric food allergy dietitian can help pinpoint potential nutrition concerns and help increase variety in their diet.
I am a pediatric food allergy dietitian in Iowa with experience helping children with feeding concerns. Click here to schedule an appointment with me.
Want to save this article? Click here to download a PDF copy and get more food allergy nutrition tips delivered to your inbox.